Ameriben Prior Authorization Fax Form
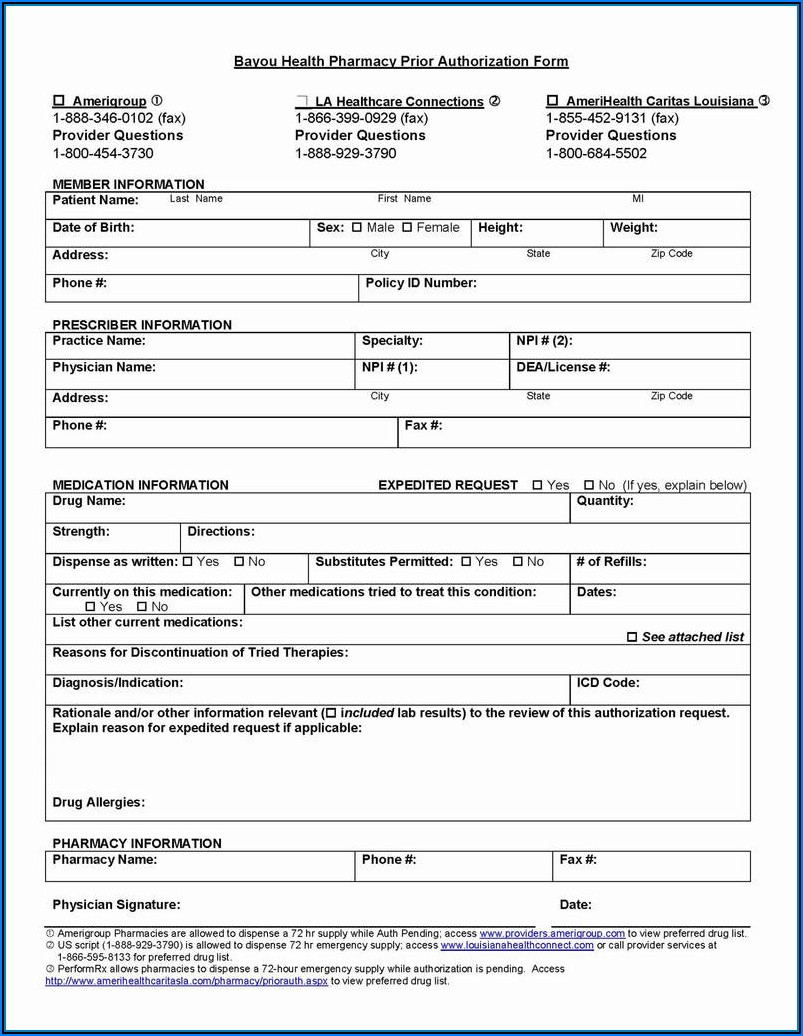
Ameriben Prior Authorization Fax Form - Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. To submit the ameriben precertification fax request form, fax it to the designated number: Benefits quoted here are a general description and not a guarantee of payment. Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care.
Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. To submit the ameriben precertification fax request form, fax it to the designated number: Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and not a guarantee of payment.
Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and not a guarantee of payment. To submit the ameriben precertification fax request form, fax it to the designated number: Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care.
Ameriben Prior Authorization Form
Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and not a guarantee of payment. Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. To submit the ameriben precertification fax request form, fax.
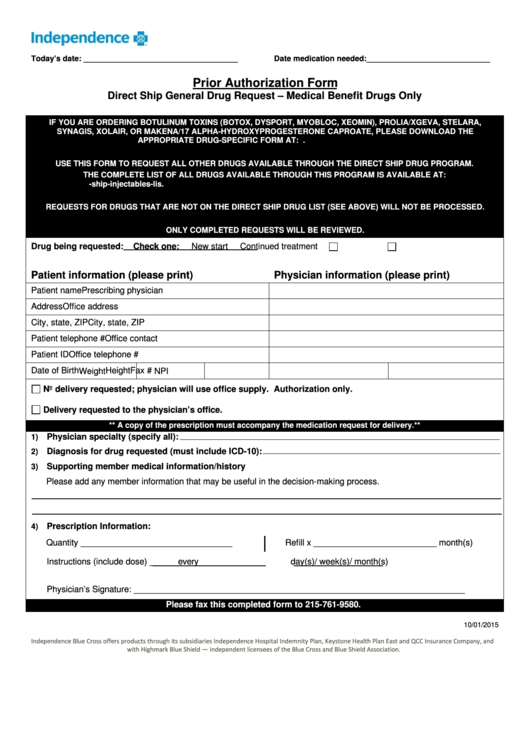
Prior Authorization Form Independence Blue Cross printable pdf download
Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Benefits quoted here are a general description and not a guarantee of payment. To submit the ameriben precertification fax request form, fax it to the designated number: Please see ameriben's continuity of care coverage request form to review frequently asked questions.

20202024 Sunshine Health Inpatient Medicaid Prior Authorization Fax
Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. To submit the ameriben precertification fax request form, fax it to the designated number: Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Benefits quoted here are a general description and.

Ameriben Authorization Form Fill Online, Printable, Fillable, Blank
Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and not a guarantee of payment. To submit the ameriben precertification fax request form, fax.

Fillable Online Ameriben Medical Management Prior Authorization Form
To submit the ameriben precertification fax request form, fax it to the designated number: Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Benefits quoted here are a general description and.

ameriben solutions provider portal
To submit the ameriben precertification fax request form, fax it to the designated number: Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and.

Fillable Online Ameriben precert fax form Fax Email Print pdfFiller
Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Benefits quoted here are a general description and not a guarantee of payment. To submit the ameriben precertification fax request form, fax it to the designated number: Please see ameriben's continuity of care coverage request form to review frequently asked questions.
Fillable Online Ameriben Prior Authorization Form Pdf Fax Email Print
Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. To submit the ameriben precertification fax request form, fax it to the designated number: Benefits quoted here are a general description and.

Fillable Online Ameriben Authorization Form STUDIO ALESSANDRETTI .it
Benefits quoted here are a general description and not a guarantee of payment. Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. To submit the ameriben precertification fax request form, fax it to the designated number: Please see ameriben's continuity of care coverage request form to review frequently asked questions.
Ameriben Precertification Fax Request You can work Doc Template
Each plan may require precertification (prior authorization with review of medical necessity) of certain medical and/or surgical health care. Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of. Benefits quoted here are a general description and not a guarantee of payment. To submit the ameriben precertification fax request form, fax.
Each Plan May Require Precertification (Prior Authorization With Review Of Medical Necessity) Of Certain Medical And/Or Surgical Health Care.
To submit the ameriben precertification fax request form, fax it to the designated number: Benefits quoted here are a general description and not a guarantee of payment. Please see ameriben's continuity of care coverage request form to review frequently asked questions or to request continuity of.