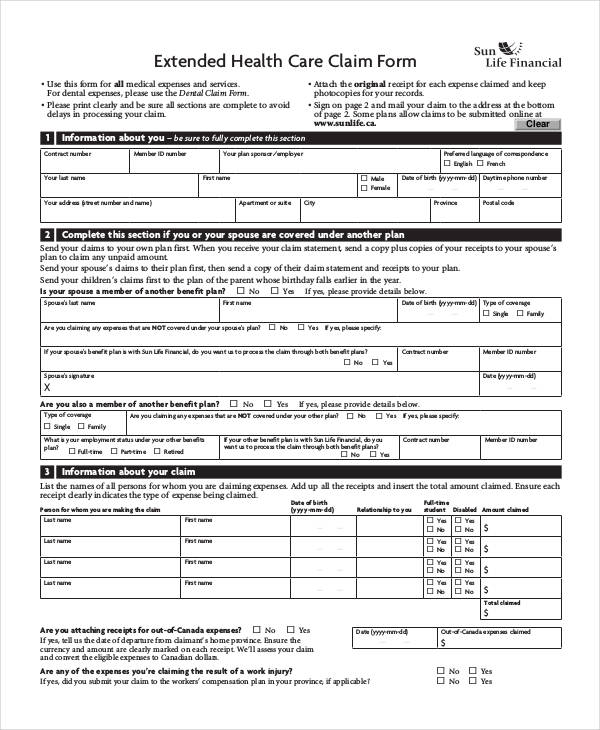
Facility Claim Form
Facility Claim Form - Policy form numbers and product availability vary by state. Claim form, signed, and dated by the policyholder or their representative. If a legal representative completes and. This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters.
If a legal representative completes and. This number will be printed on the. Claim form, signed, and dated by the policyholder or their representative. Policy form numbers and product availability vary by state. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters.
This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. Policy form numbers and product availability vary by state. Claim form, signed, and dated by the policyholder or their representative. If a legal representative completes and.

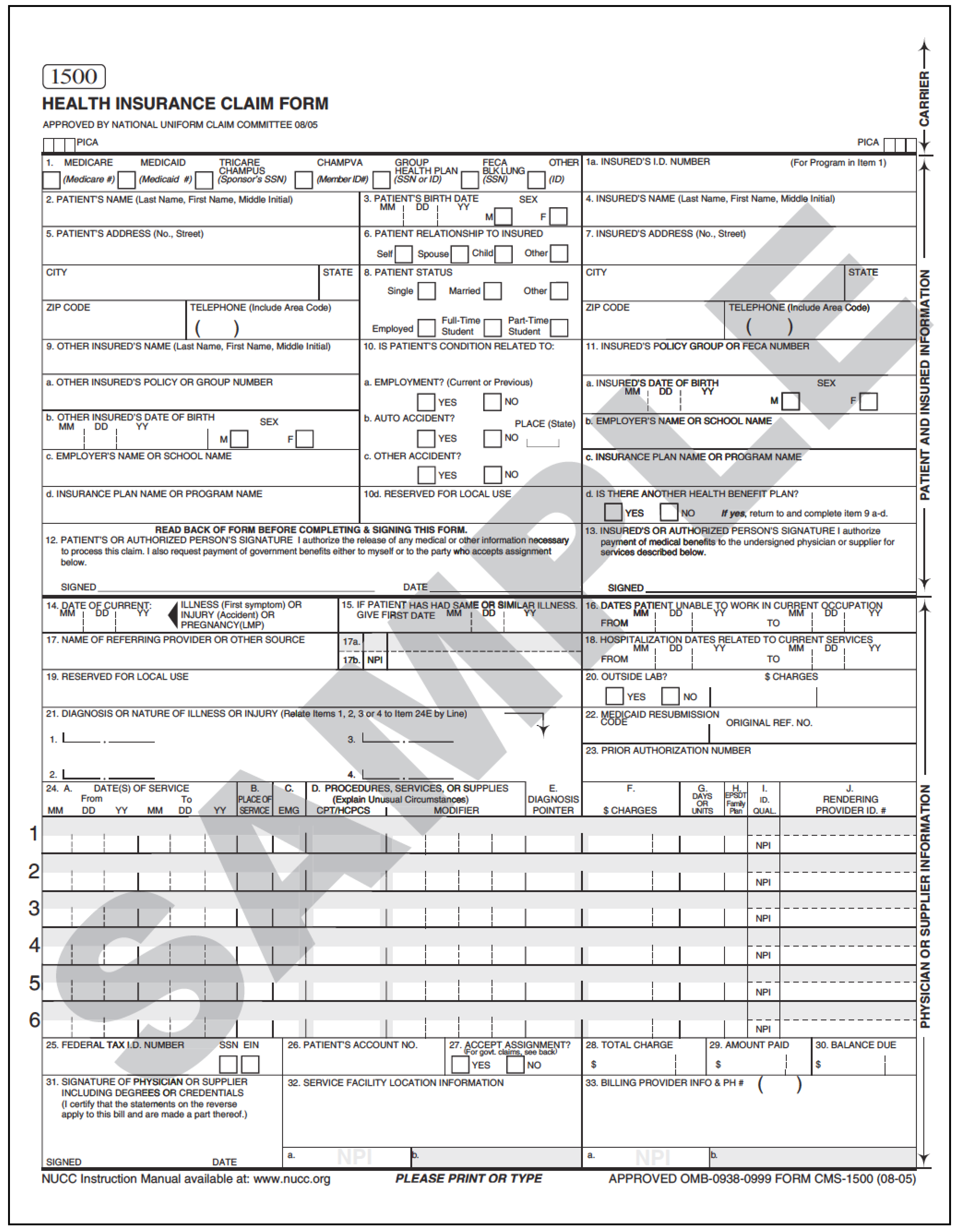
ComplyRight™ CMS1500 Health Insurance Claim Form (02/12), Laser Cut
This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. If a legal representative completes and. Claim form, signed, and dated by the policyholder or their representative. Policy form numbers and product availability vary by state.
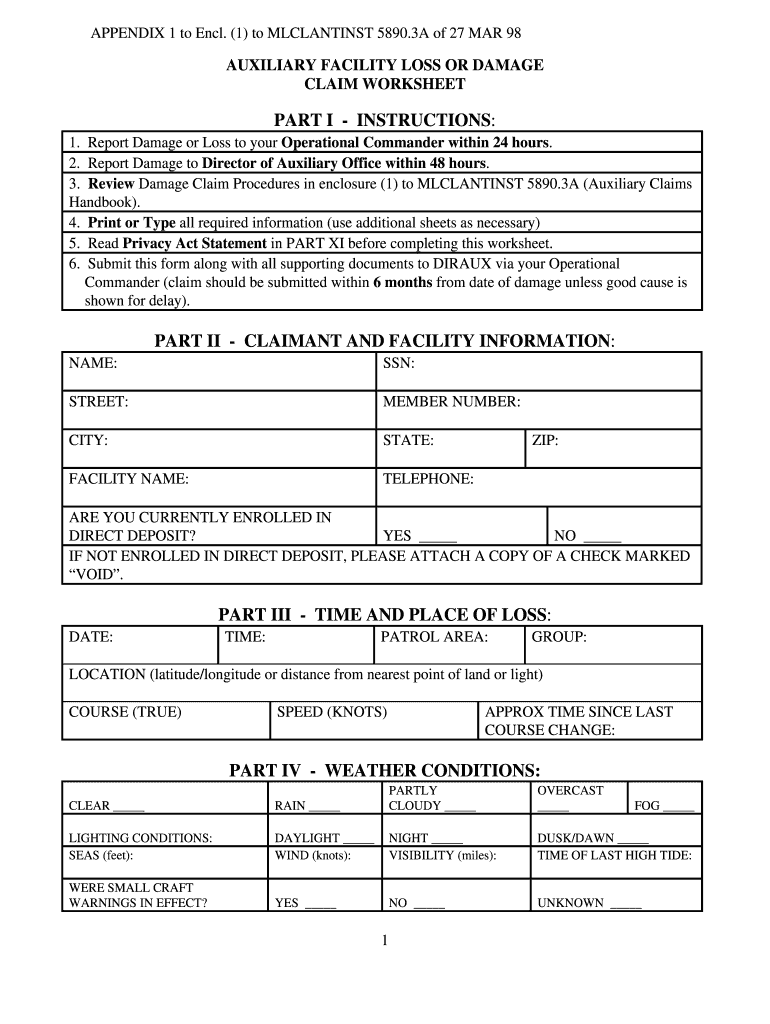
Facility claim worksheet form Fill out & sign online DocHub
If a legal representative completes and. This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. Claim form, signed, and dated by the policyholder or their representative. Policy form numbers and product availability vary by state.

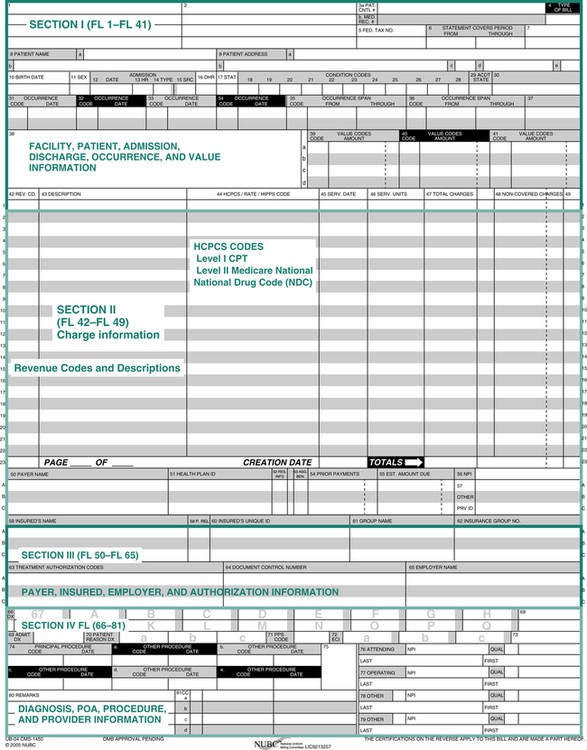
Free Fillable Ub 04 Claim Form Printable Forms Free Online
If a legal representative completes and. Policy form numbers and product availability vary by state. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. This number will be printed on the. Claim form, signed, and dated by the policyholder or their representative.

Hospital Claim Form
If a legal representative completes and. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. This number will be printed on the. Policy form numbers and product availability vary by state. Claim form, signed, and dated by the policyholder or their representative.
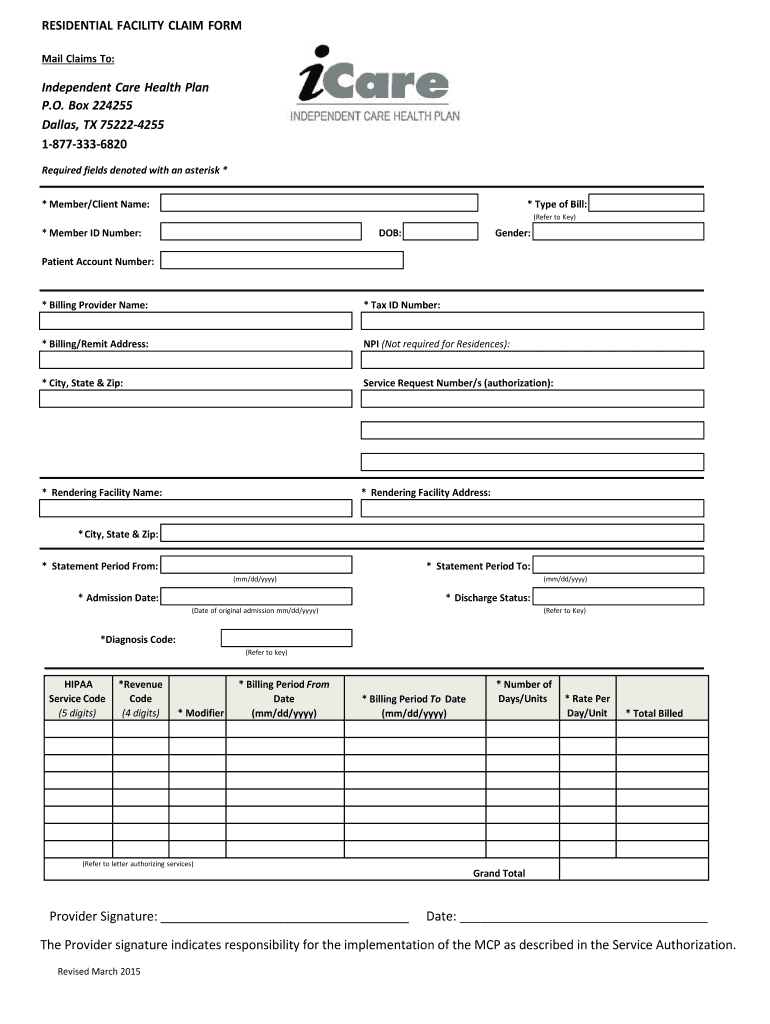
Fillable Online icarewi RESIDENTIAL FACILITY CLAIM FORM Fax Email
If a legal representative completes and. Claim form, signed, and dated by the policyholder or their representative. Policy form numbers and product availability vary by state. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. This number will be printed on the.
Claim Forms Nurse Key
Policy form numbers and product availability vary by state. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. If a legal representative completes and. Claim form, signed, and dated by the policyholder or their representative. This number will be printed on the.
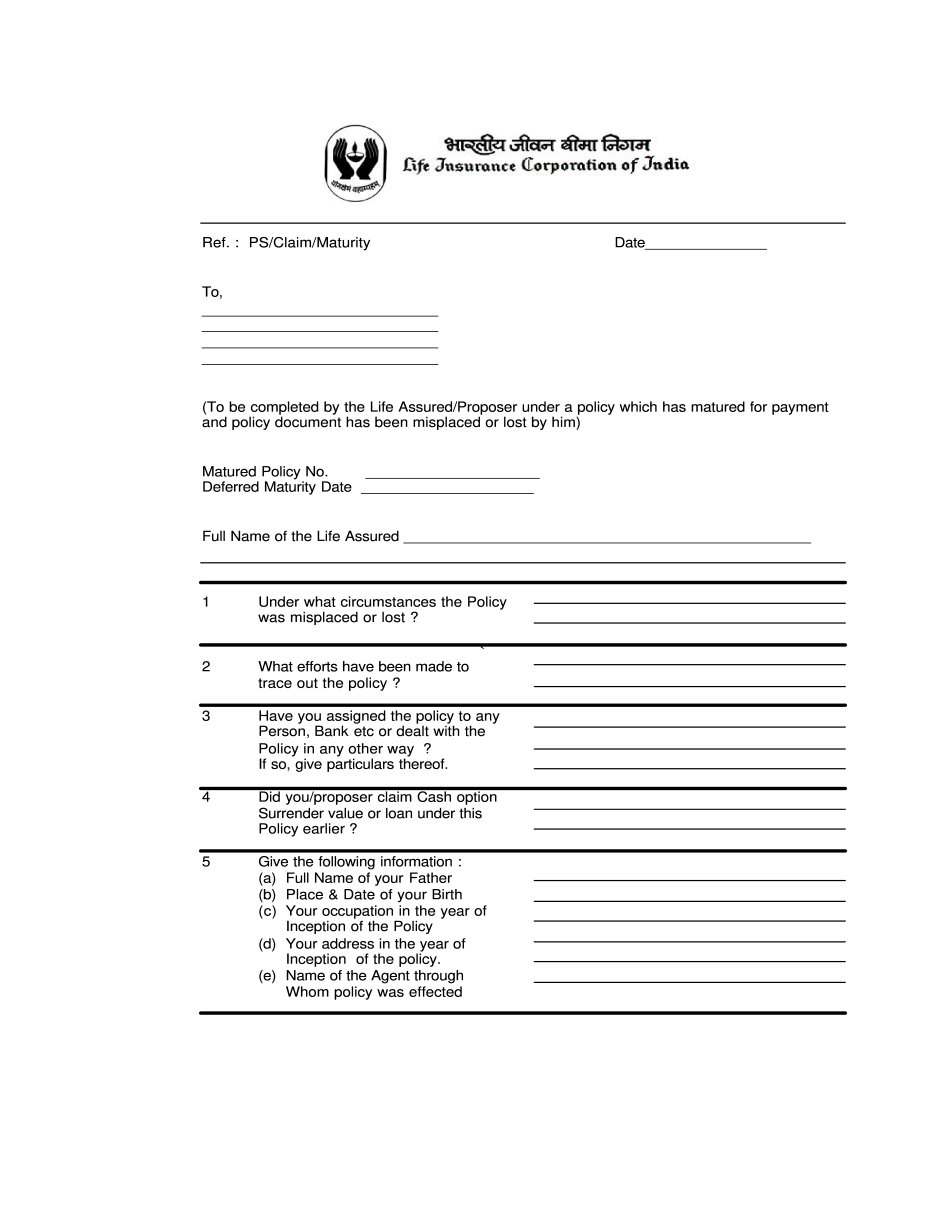
Manage Documents Using Our Editable Form For LIC Claim Form
Claim form, signed, and dated by the policyholder or their representative. This number will be printed on the. Policy form numbers and product availability vary by state. If a legal representative completes and. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters.
CMS1500 (Professional Paper Claim Form) to ANSI 837 Electronic Claim
Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. This number will be printed on the. Claim form, signed, and dated by the policyholder or their representative. If a legal representative completes and. Policy form numbers and product availability vary by state.
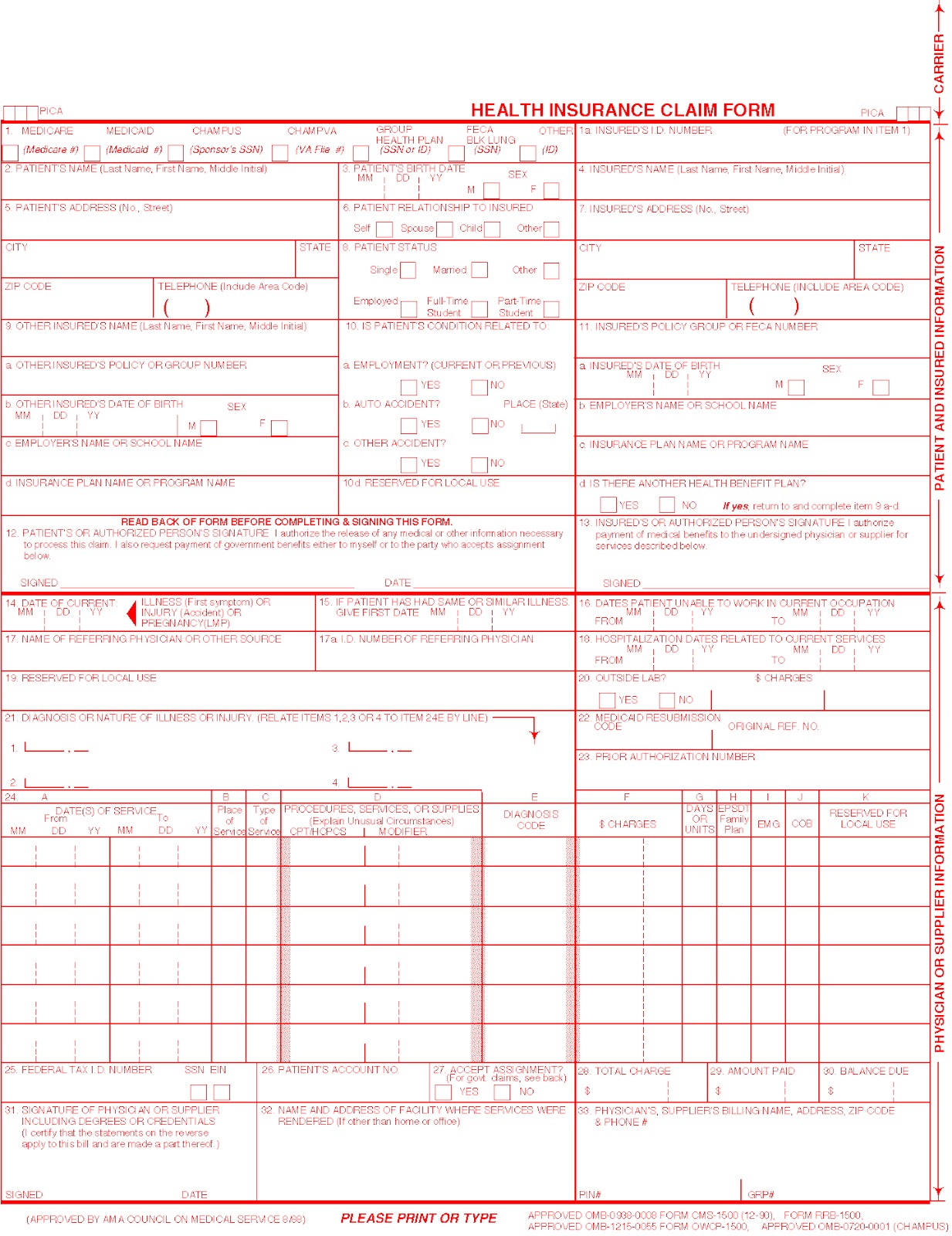
Fillable Hcfa 1500 Claim Form Printable Forms Free Online
Claim form, signed, and dated by the policyholder or their representative. This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters. If a legal representative completes and. Policy form numbers and product availability vary by state.
FREE 40+ Claim Forms in PDF Excel MS Word
If a legal representative completes and. Policy form numbers and product availability vary by state. Claim form, signed, and dated by the policyholder or their representative. This number will be printed on the. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters.
Policy Form Numbers And Product Availability Vary By State.
If a legal representative completes and. This number will be printed on the. Claim form, signed, and dated by the policyholder or their representative. Enter your facility's unique account number assigned to the patient, up to 20 alpha/numeric characters.