Indiana Healthcare Representative Form
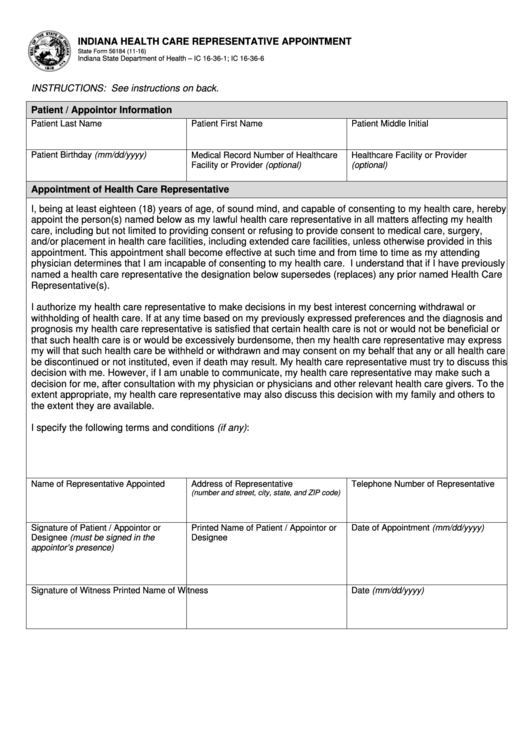
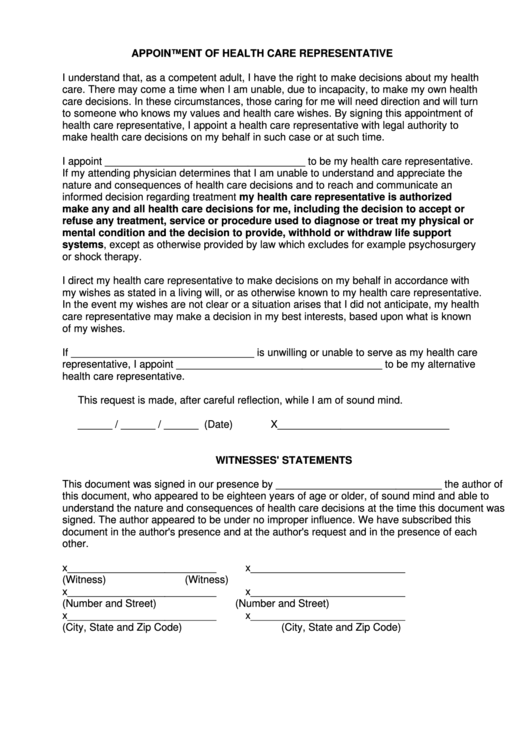
Indiana Healthcare Representative Form - Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I, ___________________________________, voluntarily appoint the following person as my health care representative. I, _____, give my hcr named below permission to make health care. A representative may be a parent of a. Appointment of health care representative: The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care.
Appointment of health care representative: A representative may be a parent of a. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I, _____, give my hcr named below permission to make health care. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. I, ___________________________________, voluntarily appoint the following person as my health care representative. The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care.
The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. I, _____, give my hcr named below permission to make health care. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. A representative may be a parent of a. Appointment of health care representative: I, ___________________________________, voluntarily appoint the following person as my health care representative.
Indiana Medicaid Authorized Representative Form Complete with ease
The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. A representative may be a parent of a. I, ___________________________________, voluntarily appoint the following person as my health care representative. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of.

Moving to Indiana Pros & Cons (Truth About Living in 2022)
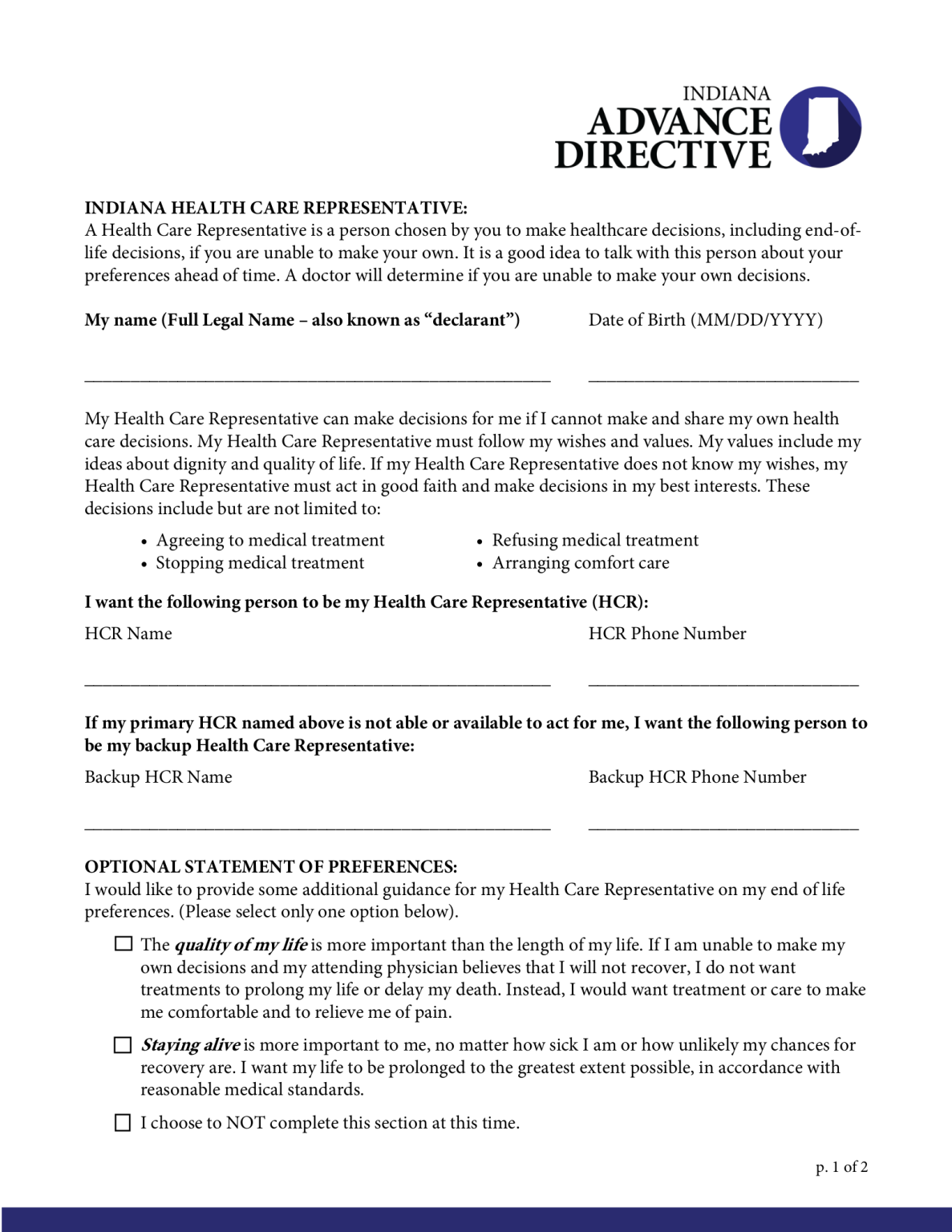
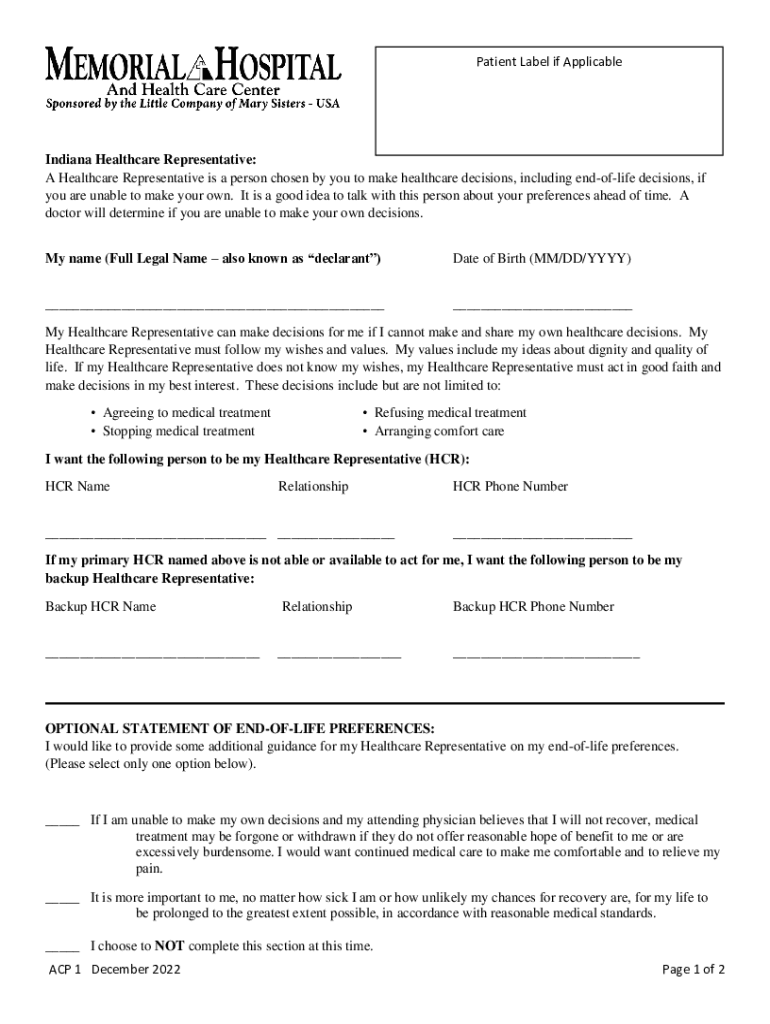
I, _____, give my hcr named below permission to make health care. A representative may be a parent of a. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. I, ___________________________________, voluntarily appoint the following person as my health care representative. Appointment of health care representative:
391 Indiana Legal Forms And Templates free to download in PDF
If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost.
Free Indiana Medical Power of Attorney PDF eForms
The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. A representative may be a parent of a. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I, ___________________________________, voluntarily appoint the following person as my health care representative. Appointment of health.
Fillable Online Indiana Medical Power of Attorney (Form 56184) eForms
I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care. I, _____, give my hcr named below permission to make health care. A representative may be a parent of a. The post form may be completed by a patient, or if applicable, a patient’s legal.
Fillable Online Templates to Appoint Healthcare Representative Form Fax
A representative may be a parent of a. Appointment of health care representative: I, ___________________________________, voluntarily appoint the following person as my health care representative. I, _____, give my hcr named below permission to make health care. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the.
Health Care Proxy Forms Printable
Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care. The post form may be completed by a patient, or if applicable, a patient’s legal representative.

Blank Authorized Representative Form Fill Out and Print PDFs
If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I understand that.

Veterans Affairs SPS Addition, VA Northern Indiana Healthcare System
Appointment of health care representative: Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care. If you want someone to represent you concerning services received under.
Fillable Online Authorization of Representative Form July 2023
Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care. The post form may be completed by a patient, or if applicable, a patient’s legal representative or proxy. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the.
I, ___________________________________, Voluntarily Appoint The Following Person As My Health Care Representative.
I, _____, give my hcr named below permission to make health care. If you want someone to represent you concerning services received under medicaid, including the sharing of your protected health information,. I understand that a family member as a health care representative, in that capacity, incurs no personal liability for the cost of the health care. Authorize my health care representative to make decisions in my best interest concerning withdrawal or withholding of health care.
The Post Form May Be Completed By A Patient, Or If Applicable, A Patient’s Legal Representative Or Proxy.
Appointment of health care representative: A representative may be a parent of a.