Medicaid Authorized Representative Form
Medicaid Authorized Representative Form - A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. Division of budget and analysis. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: The ar and the person applying. The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf.
Division of budget and analysis. The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. The ar and the person applying. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section:
The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. Division of budget and analysis. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: The ar and the person applying. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be.
Indiana Medicaid Authorized Representative Form Complete with ease
The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: Division of budget and analysis. A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi).
New Jersey Medicaid Authorized Form Fill Online, Printable, Fillable
A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. Division of budget.
2023 Marketplace Pa Guide Request Form Printable Forms Free Online
Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. The ar and the person applying. Designation of authorized representative if the health choice recipient is under age 18, please fill.
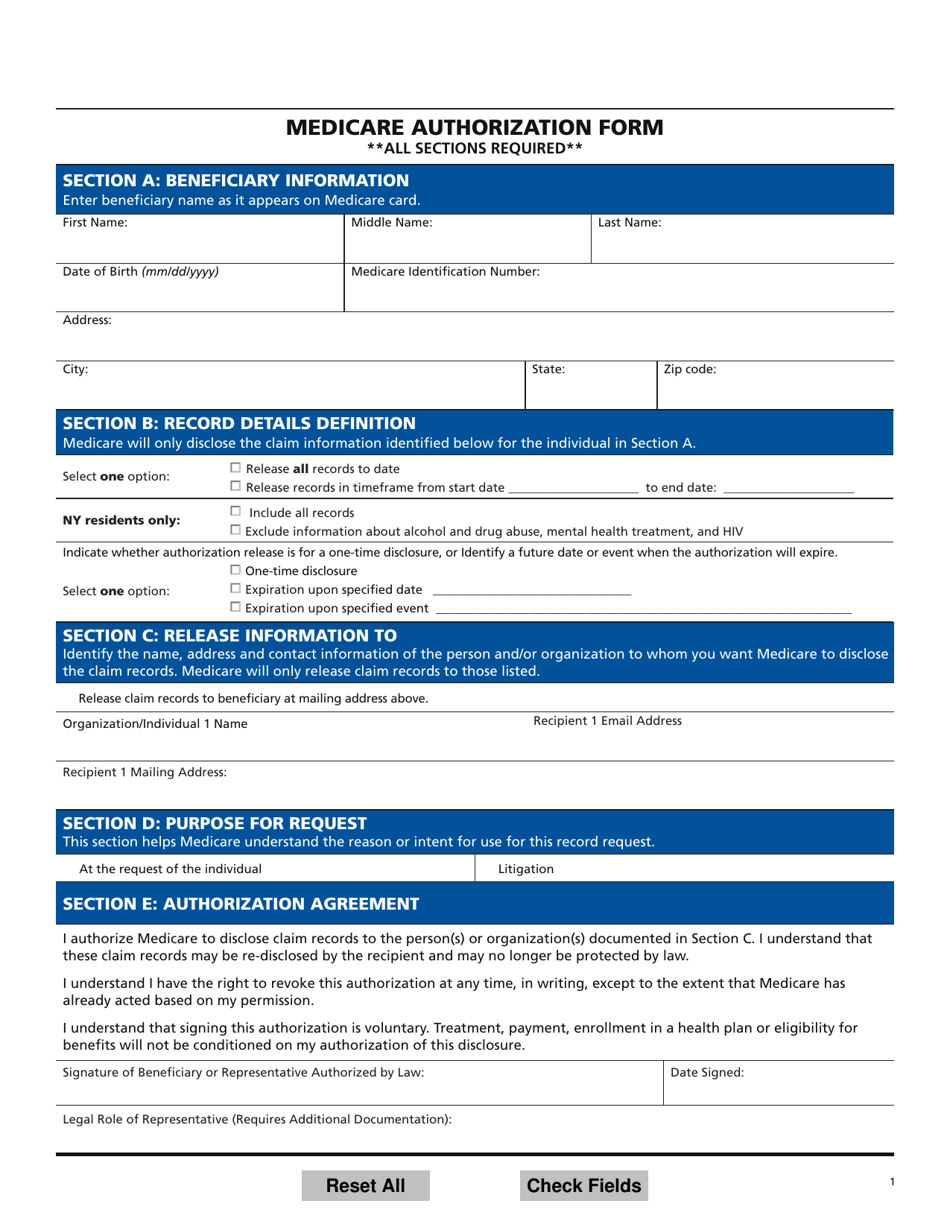
Medicare Authorization Form Fill Out, Sign Online and Download PDF
The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. A.
Bcbs standard authorization form Fill out & sign online DocHub
A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. The ar and the person applying. The purpose of the authorized representative information screen is to assure that authorized representatives receive.
Odm 06723 20172024 Form Fill Out and Sign Printable PDF Template
A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. The ar and the person applying. Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: Division of budget and analysis. This form allows you to give a trusted person permission.
Fillable Online Indiana Medicaid Authorized Representative Form Fax
Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be. The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. The ar and.
Fillable Form Dss1688 Designation Of Authorized Representative
Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. The ar and the person applying. Division of budget and analysis. Any individual who is legally authorized or designated in writing by the applicant/beneficiary.
Medicaid authorized representative form Fill out & sign online DocHub
The ar and the person applying. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. A person applying for medicaid or a beneficiary can choose someone they trust.

Free New York Medicaid Prior Authorization Form PDF eForms
Designation of authorized representative if the health choice recipient is under age 18, please fill out this section: This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf. A.
Division Of Budget And Analysis.
The purpose of the authorized representative information screen is to assure that authorized representatives receive medicaid and special. The ar and the person applying. This form allows you to give a trusted person permission to act for you on matters related to your medicaid application or case. Any individual who is legally authorized or designated in writing by the applicant/beneficiary (a/b) to act on behalf.
Designation Of Authorized Representative If The Health Choice Recipient Is Under Age 18, Please Fill Out This Section:
A person applying for medicaid or a beneficiary can choose someone they trust with their protected health information (phi) to be.