Medical Record Release Form Pdf
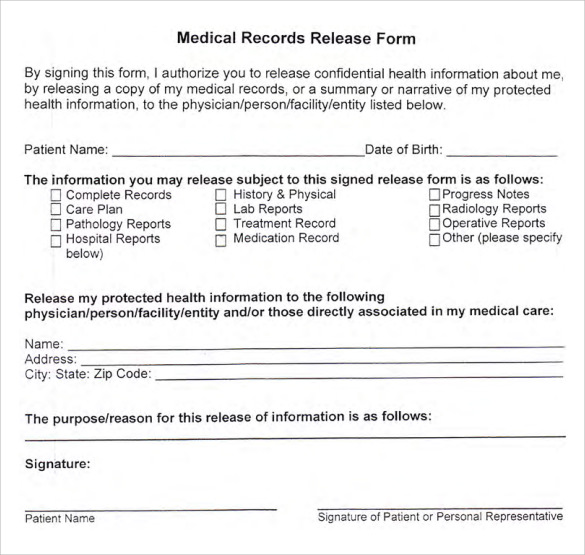
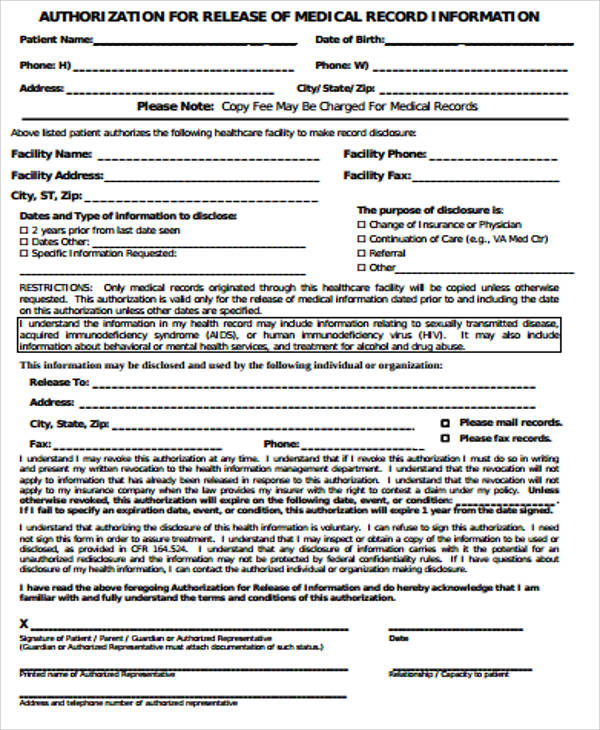
Medical Record Release Form Pdf - Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. A patient can also request their medical records. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. Specific information to be released: A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Please complete all sections of this hipaa release form. _____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or information.
Specific information to be released: A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. _____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or information. If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Please complete all sections of this hipaa release form. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. A patient can also request their medical records. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of.
Specific information to be released: Please complete all sections of this hipaa release form. If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. _____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or information. A patient can also request their medical records.

Free Medical Release Form Template Continuum
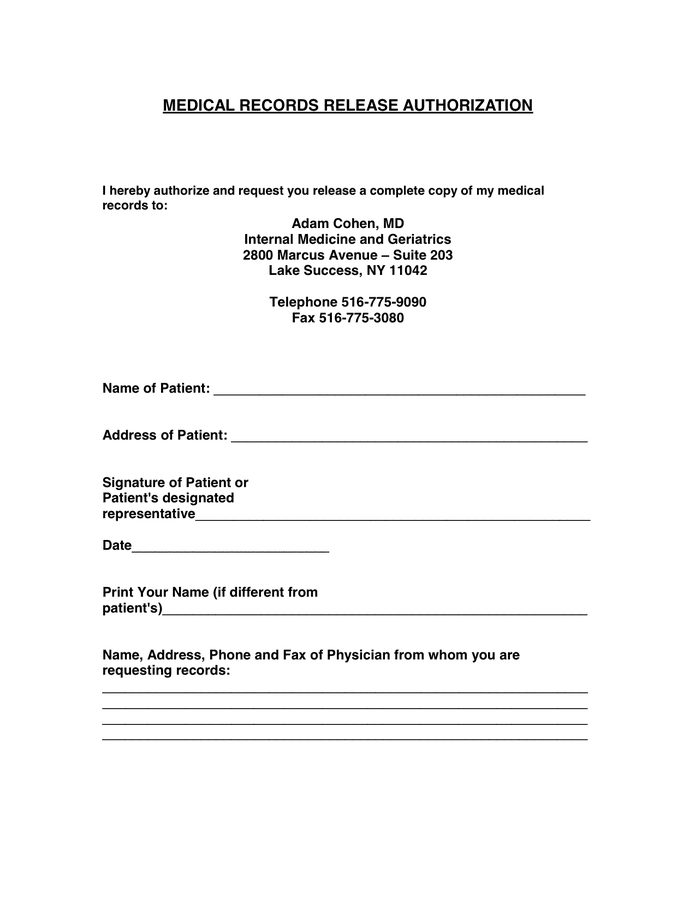
_____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or information. Please complete all sections of this hipaa release form. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. A patient can also request their medical.
FREE 9+ Sample Medical Records Release Forms in PDF
A patient can also request their medical records. Specific information to be released: Please complete all sections of this hipaa release form. If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Q entire medical record, including patient histories, office notes (except psychotherapy notes),.
MEDICAL RECORDS RELEASE AUTHORIZATION in Word and Pdf formats
Specific information to be released: Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. A patient can also request their medical records. _____ if such information exists, i.
FREE 32+ Medical Release Form Samples, PDF, MS Word, Google Docs
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Please complete all sections of this hipaa release form. Specific information to be released: A medical records release authorization form is a document that allows a person to disclose protected health information to a.
FREE 9+ Medical Record Release Form Samples in MS Word PDF
Please complete all sections of this hipaa release form. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. _____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or information. If any sections are left blank, this.
FREE 9+ Sample Medical Records Release Forms in PDF
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. Please complete all sections of this hipaa release form. Specific information to be released: To.

Medical Release Form Template Complete with ease airSlate SignNow
A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. Please complete all sections of this hipaa release form. Specific information to be released: Q entire medical record, including.

Medical Record Release form Lovely Sample Medical Records Release form
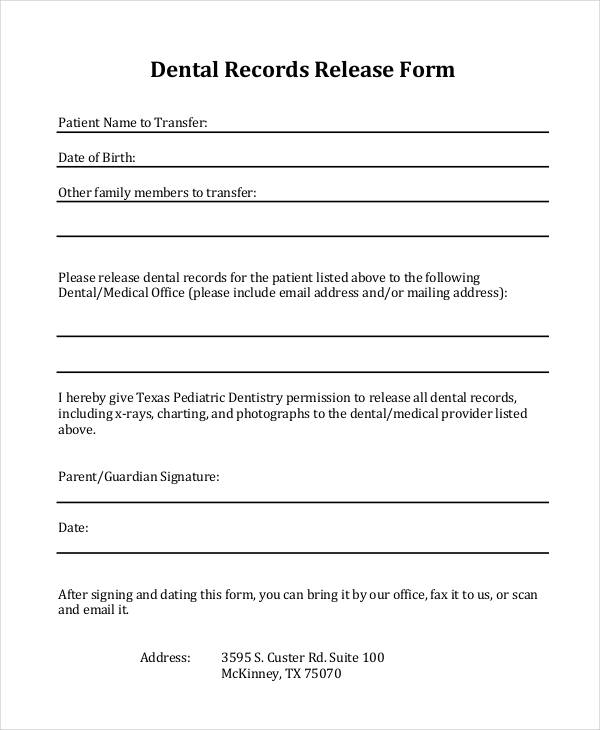
Please complete all sections of this hipaa release form. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,. A patient can also request their medical records. _____ if such information exists, i authorize the disclosure of the entire medical record or the following specifi c documents, dates of service, and/or.
Medical Record Request Template
To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. Specific information to be released: If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. A patient can also request their medical records. _____ if.
Medical Records Release Form in Word and Pdf formats
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Please complete all sections of this hipaa release form. A patient can also request their medical records. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films,.
_____ If Such Information Exists, I Authorize The Disclosure Of The Entire Medical Record Or The Following Specifi C Documents, Dates Of Service, And/Or Information.
A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Specific information to be released: To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of. Q entire medical record, including patient histories, office notes (except psychotherapy notes), test results, radiology studies, films, referrals, consults,.
A Patient Can Also Request Their Medical Records.
Please complete all sections of this hipaa release form. If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested.