Personal Representative Designation Form
Personal Representative Designation Form - Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. Designate a personal representative if you would like another person to act on your behalf when discussing your health care. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to.
Designate a personal representative if you would like another person to act on your behalf when discussing your health care. Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to.
Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. Designate a personal representative if you would like another person to act on your behalf when discussing your health care. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. I hereby designate the following personal representative to assist me in exercising my health information rights under the new.
Oath of Personal Representative & Designation & Acceptance of Resident
I hereby designate the following personal representative to assist me in exercising my health information rights under the new. Designate a personal representative if you would like another person to act on your behalf when discussing your health care. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative,.

AllWays Health Partners Authorized Personal Representative Designation
I hereby designate the following personal representative to assist me in exercising my health information rights under the new. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. Designate a personal representative if you would like another person to act on your behalf when.
I Am the Personal Representative in This Estate Form Fill Out and
Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. If.

Fillable Online Personal Representative Designation Form General
I hereby designate the following personal representative to assist me in exercising my health information rights under the new. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. As required by the health information portability and accountability act (hipaa) privacy rule, you have a.

Fillable Online Notice of Personal Healthcare Representative
If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a.
PERSONAL REPRESENTATIVE1 Form Fill Out and Sign Printable PDF
I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to.

Fillable Online Designation of Personal Representative. Designation of
Designate a personal representative if you would like another person to act on your behalf when discussing your health care. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and.

Upmc Health Plan Personal Representative Designation Form
Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. If.

CA personal representative form Fill and Sign Printable Template
Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. Designate a personal representative if you would like another person to act on your behalf when discussing your health care. I hereby designate the following personal representative to assist me in exercising my health information rights under the.
Fillable Online Personal Representative Designation for Protected
As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to. Designate a personal representative if you would like another person to act on your behalf when discussing your health care. Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited..
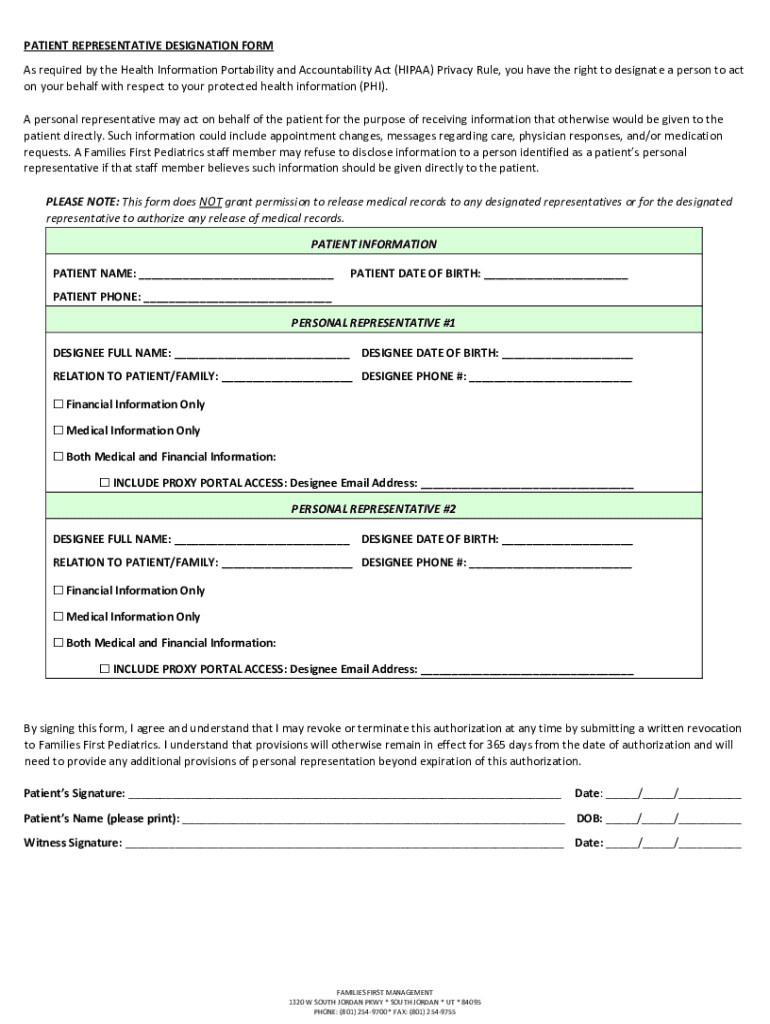
Designate A Personal Representative If You Would Like Another Person To Act On Your Behalf When Discussing Your Health Care.
Please use this form to designate a personal representative to act on your behalf in making health care related decisions and unlimited. If you sign this form, you are giving the agency permission to treat the person(s) you name as your personal representative, and to share your. I hereby designate the following personal representative to assist me in exercising my health information rights under the new. As required by the health information portability and accountability act (hipaa) privacy rule, you have a right to.