Release Of Information Form In Spanish
Release Of Information Form In Spanish - ⚫ tengo el derecho de negarme a firmar este. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family.
4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. ⚫ tengo el derecho de negarme a firmar este.
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. ⚫ tengo el derecho de negarme a firmar este. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue.
Information Release Form Template
⚫ tengo el derecho de negarme a firmar este. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form.
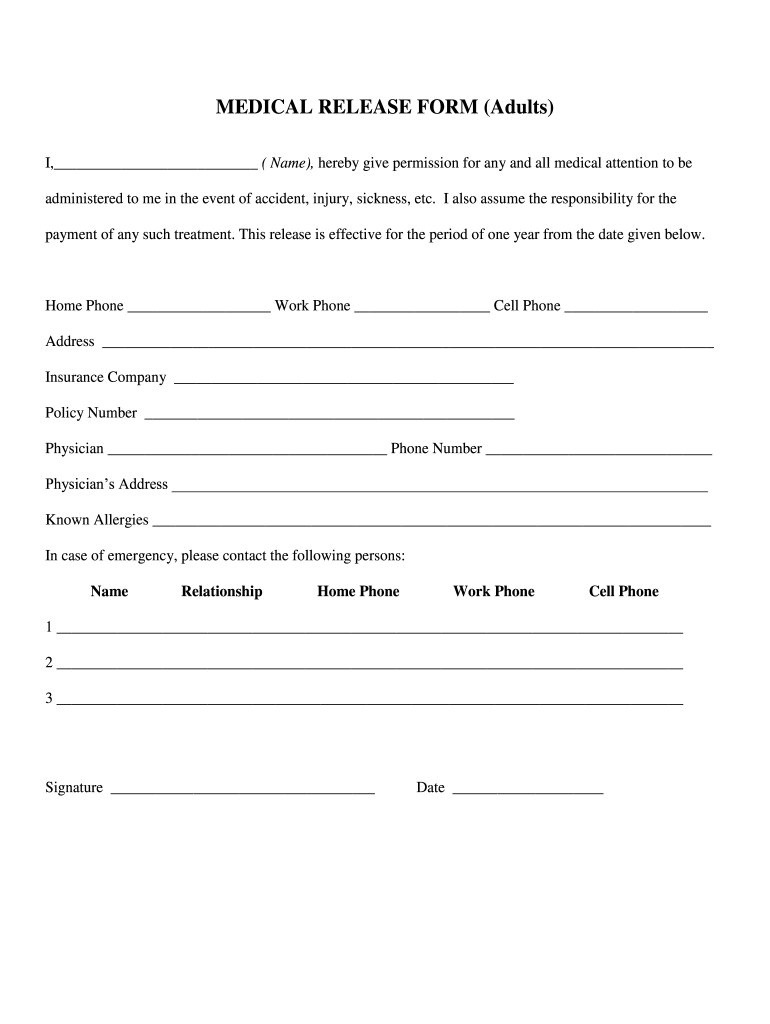
Medical Release Form Printable
Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a.
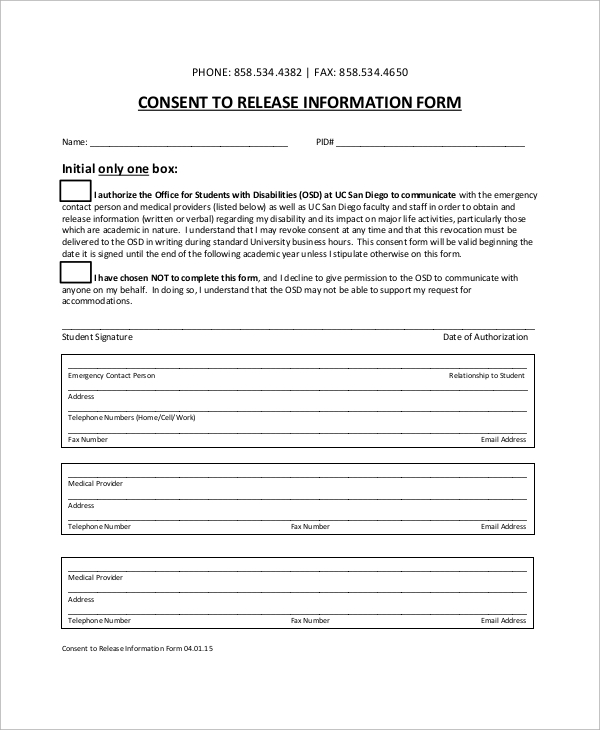
Consent Release Of Information Authorization Form
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. ⚫ tengo el derecho de negarme a firmar.
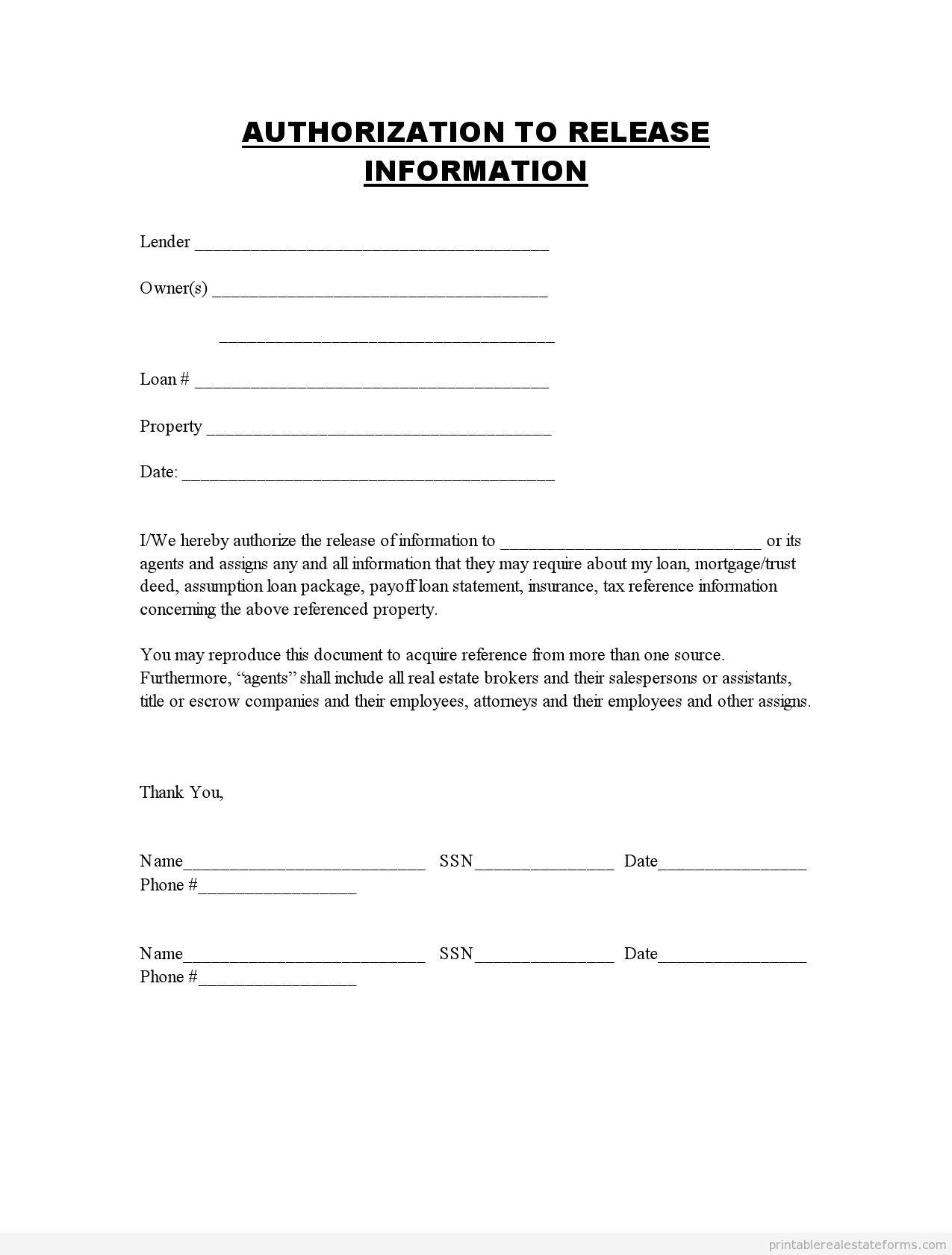
Free Authorization To Release Medical Records Form Template Word
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your.

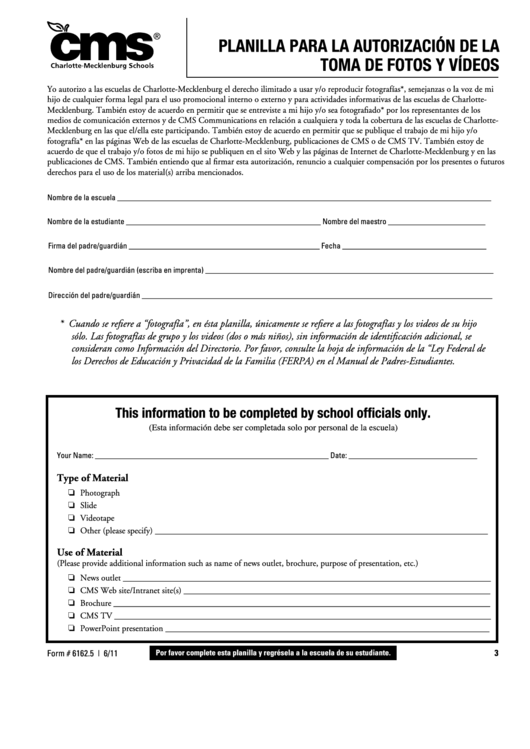
Printable Spanish Patient Registration Form Printable Forms Free Online
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. 960 autorización para divulgar información médica de conformidad con hipaa [este.

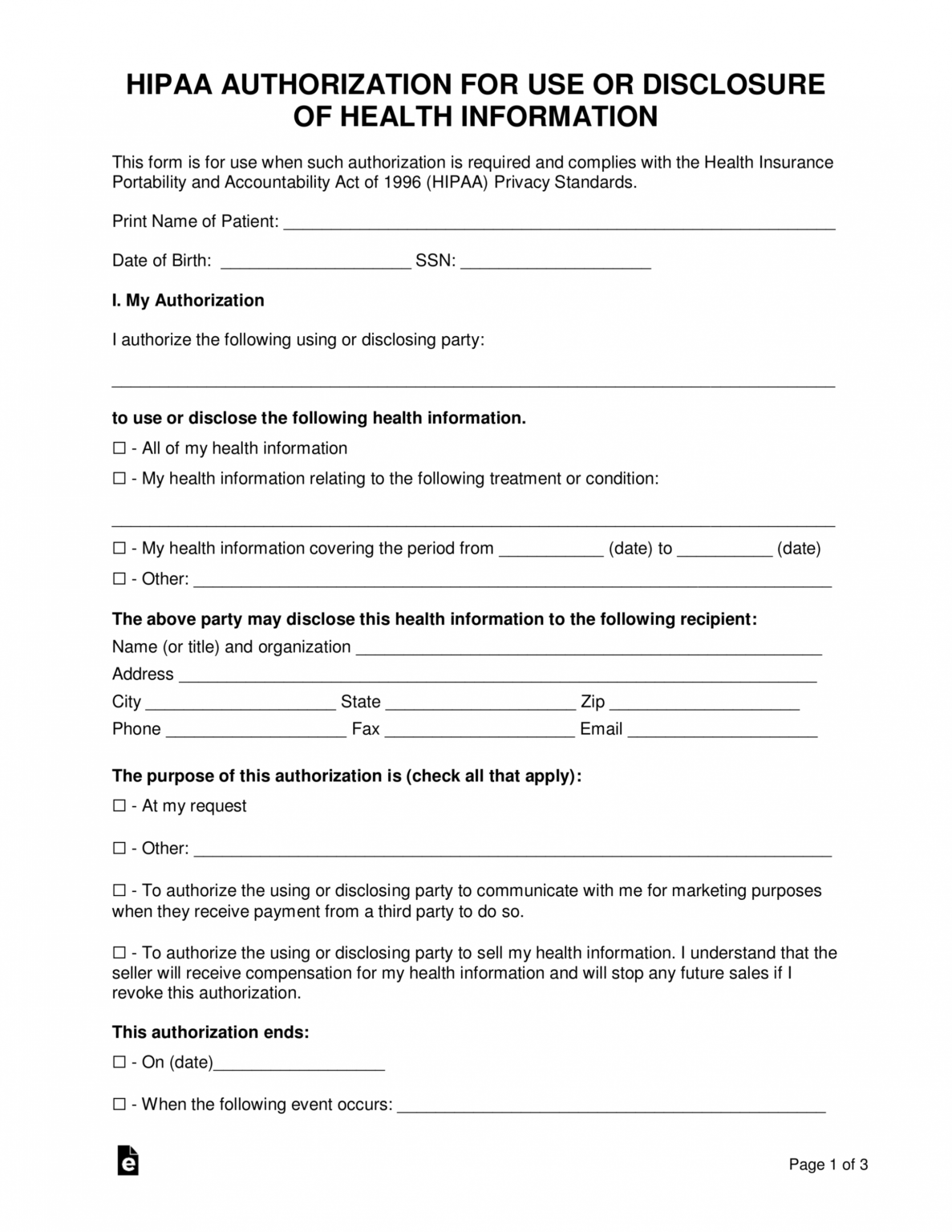
HIPAA Authorisation Form YouTube
4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. ⚫ tengo el derecho de negarme a firmar este. Authorization for release of.
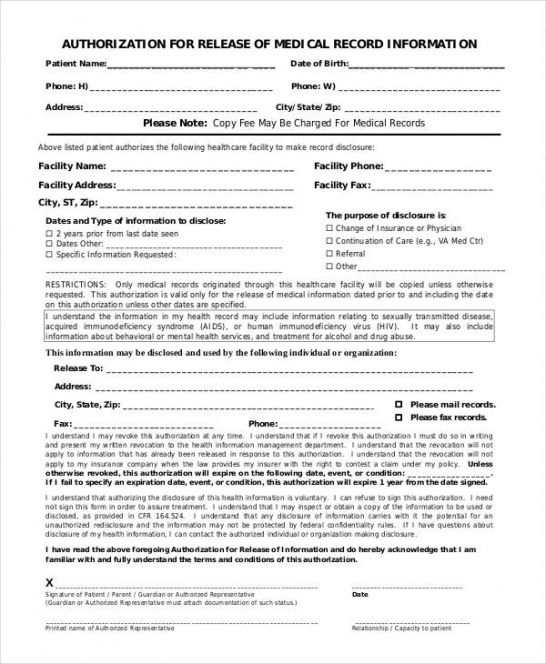
Medical Release Form 20202022 Fill and Sign Printable Template
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. ⚫ tengo el derecho de negarme a firmar este. 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. Authorization to use, disclose.
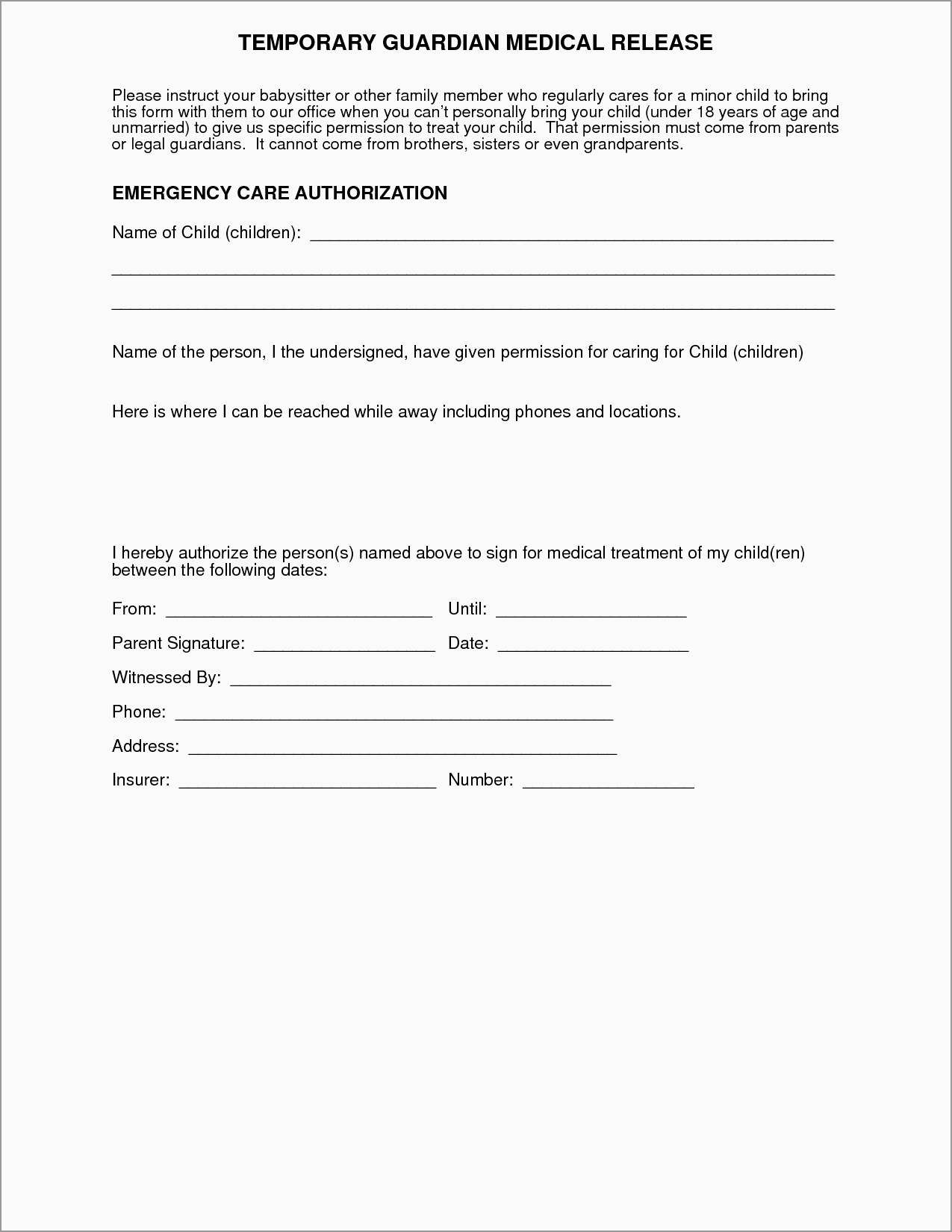
Free Printable Medical Consent Form For Trainers Printable Forms Free
⚫ tengo el derecho de negarme a firmar este. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. 960 autorización.
Top Release Form In Spanish Templates free to download in PDF format
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: ⚫ tengo el derecho de negarme a firmar este. Authorization for release of health information (spanish) authorization for release of health.
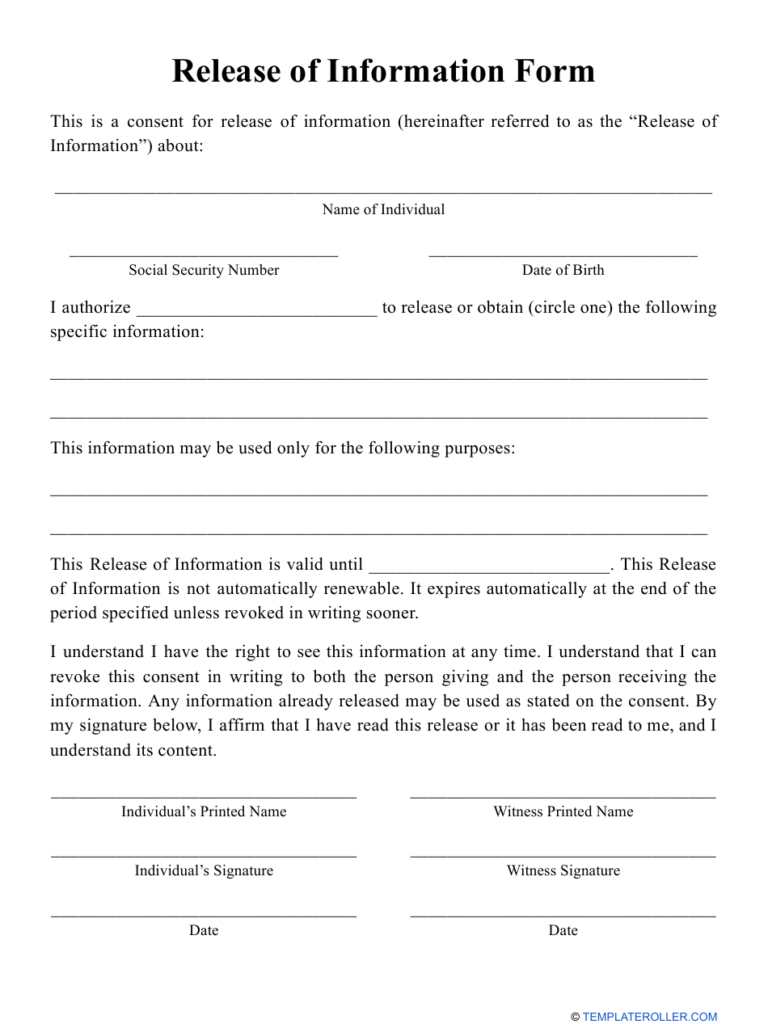
Release Of Information Form Download Printable PDF Templateroller
960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your.
4/2024 Coloque La Etiqueta Del Paciente Aquí (Solo Para Uso Interno) *Si Se Trata De Comunicación Oral, Complete La Autorización Para.
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente:
This Form Is To Be Used By A Patient Or Legal Representative To Authorize The Release Of Information To A Third Party (Other Than A Family.
⚫ tengo el derecho de negarme a firmar este.